
In vestibular rehabilitation therapy (VRT), head movement is not just a component of the treatment—it is the treatment. For clinicians treating vestibular hypofunction, the goal is clear: induce adaptation of the Vestibulo-Ocular Reflex (VOR).
However, a persistent challenge remains in the gap between what is prescribed in the clinic and what patients actually do at home. Is the patient moving their head fast enough to stimulate the vestibular system? Are they moving too fast, resulting in retinal blur that frustrates the brain rather than training it? Some clinicians use metronomes to pace their patient’s head movements, others give instructions such as “move your head as fast as you feel you can”. Neither of these methods provide objective data as to what the patient is actually doing. We can observe head movement in clinic, but most of the program has traditionally been done at home with the concept that distributed practice daily, is required.
This brings us to the critical importance of measuring head movement frequency and velocity and the role of objective biofeedback, such as that provided by the Vertigenius™ Head Sensor, in bridging the gap between prescription and outcome.
The Physiology: Chasing “Retinal Slip”
To understand why precision matters, we must revisit the mechanism of VOR adaptation. The brain does not repair the vestibular system simply because time passes; it repairs it also in response to an error signal. That error signal is retinal slip. (Mahfuz et al., 2020)
When a patient performs a gaze stabilization exercise (like VOR x1), they must move their head while keeping their eyes fixed on a target. Retinal image slip occurring during these head rotations drives the motor learning and neuroplasticity needed to improve VOR gain (Li et al., 2024).
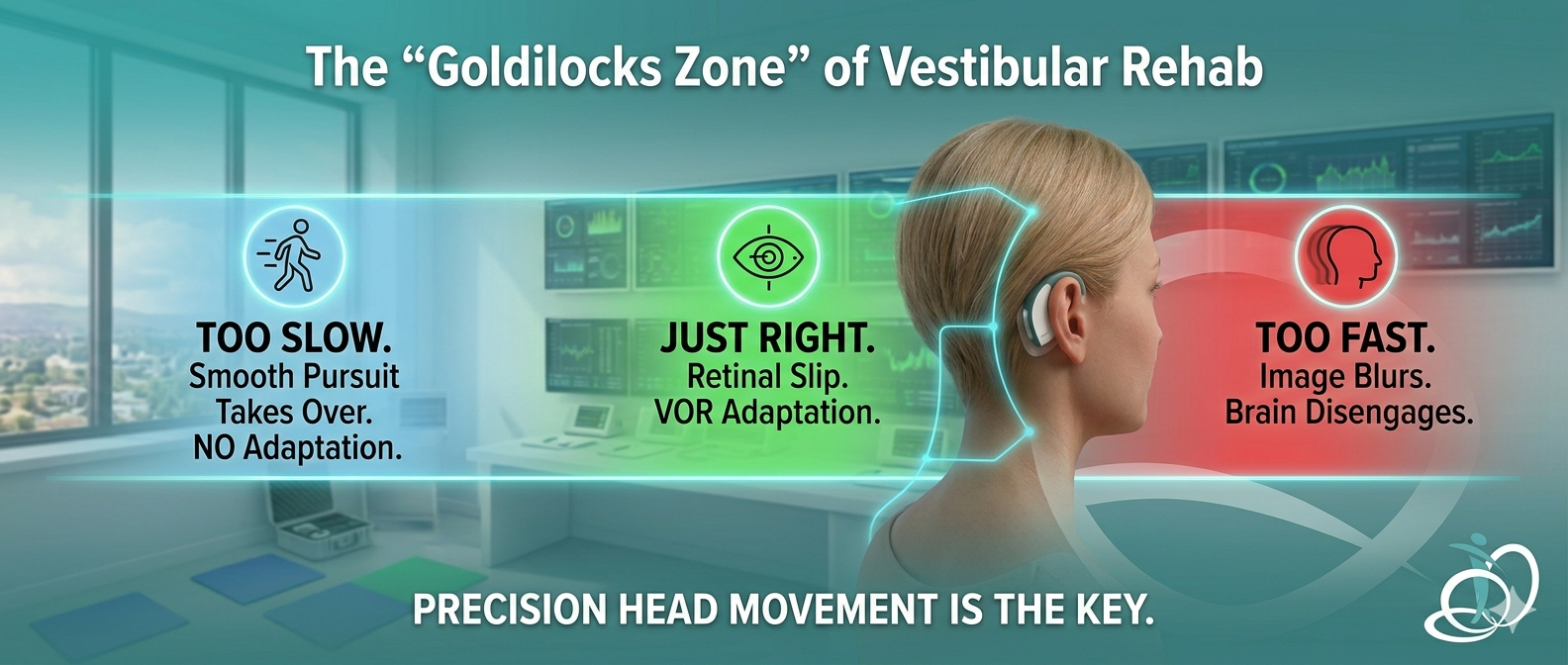
- If they move too slowly: The smooth pursuit system predominates. The vestibular system is not challenged, no error signal is generated, and likely no adaptation occurs. (Mahfuz et al., 2020)
- If they move too quickly: The image blurs completely. The brain disengages, safety anxiety and symptoms spike, and the patient may stop the exercise entirely.
There is a “Goldilocks Zone” of head velocity—typically high enough to exceed the capacity of smooth pursuit (often >100°/sec for daily function training)—where the brain registers the error and recalibrates the VOR gain. (Wang et al., 2021; Herdman & Bhatti, 2013). There is also a “Goldilocks Zone” of symptom provocation, to keep the exercise tolerable. Often measured as “don’t go above 5/10 on your symptom scale” or “don’t let your symptoms be exacerbated by more than 2-3/10 points on your symptom scale”.
The Clinical Blind Spot
Historically, ensuring a patient stays in these zones has been a game of guesswork. We tell patients, “Move your head as fast as you can while keeping the target in focus.”
But what does “fast” feel like to a patient with a vestibular disorder? To a dizzy patient, even a sluggish 30°/sec rotation can feel like a rollercoaster. Without objective feedback, patients default to safety. They slow down. They limit their range of motion. They perform “movements” that feel safe but are physiologically inadequate for rehabilitation.
This is where the Vertigenius™ Head Sensor transforms the standard of care.
From Subjective Guesswork to Objective Data
The Vertigenius™ Head Sensor removes the ambiguity of home exercise programs. By wearing the sensor during exercises, the “black box” of patient compliance is opened.
1. Real-Time Biofeedback
The sensor connects to the Vertigenius™ app, giving patients immediate, visual feedback on their performance. It guides them into the correct velocity range. If they are moving too slowly to generate retinal slip, the app prompts them to speed up. If they are erratic, it guides them to stabilize. This ensures that every minute spent exercising is a minute spent stimulating neuroplasticity. (Meldrum et al., 2024)
2. Combating Fear-Avoidance Behavior
Anxiety is a massive barrier in VRT. Patients naturally avoid movements that provoke dizziness. (Van Laer et al., 2023; Prell & Axer, 2022). However, controlled provocation is necessary for habituation. The Head Sensor gamifies this process. By focusing on the “score” or the feedback loop on their screen, patients are often distracted from their dizziness, allowing them to push into ranges of motion and velocities they would otherwise avoid.
3. Remote Monitoring for Clinicians
For the clinician, the Vertigenius™ clinician portal provides a window into the patient’s home. You no longer have to ask, “Did you do your exercises?” The data is there. You can see:
- Compliance: Did they do the session?
- Quality: Did they achieve the target head velocity?
- Progression: Is their range of motion improving over time?
- Symptoms: What was the effect of an individual exercise on their symptoms (scored with a numerical rating scale before and after the exercise)
The Future is Measurable
The vestibular community has historically been embedded in evidence-based practice, and has robust science underpinning exercise approaches.The phrase “move your head” is no longer a sufficient instruction. We can now measure head velocity, amplitude, and frequency, as well as symptom burden during exercise, and prescribe exercise intensity with precision, just as a physician prescribes the dosage of a medication.
The Vertigenius™ Head Sensor is the tool that allows us to verify that dosage. By quantifying head movement, we empower patients to take control of their recovery and equip clinicians with the data needed to drive better, faster outcomes.
Are you ready to stop guessing and start measuring?
References
Bowman, T., Gervasoni, E., Arienti, C., Lazzarini, S., Negrini, S., Crea, S., Cattaneo, D., & Carrozza, M. (2021). Wearable Devices for Biofeedback Rehabilitation: A Systematic Review and Meta-Analysis to Design Application Rules and Estimate the Effectiveness on Balance and Gait Outcomes in Neurological Diseases. Sensors, 21(10), 3444. https://doi.org/10.3390/s21103444 Cited by: 153
Herdman, S. J., & Bhatti, P. T. (2013). A Prototype Head-Motion Monitoring System for In-Home Vestibular Rehabilitation Therapy. Journal of Bioengineering and Biomedical Sciences. https://doi.org/10.4172/2155-9538.s1-009 Cited by: 11
Li, Q., Xu, H., Chen, W., Su, A., Fu, M. J., & Walker, M. F. (2024). Short-term learning of the vestibulo-ocular reflex induced by a custom interactive computer game. Journal of Neurophysiology, 131, 16–27. https://doi.org/10.1152/jn.00130.2023 Cited by: 8
Mahfuz, M. M., Schubert, M. C., Figtree, W. V. C., & Migliaccio, A. A. (2020). Retinal Image Slip Must Pass the Threshold for Human Vestibulo-Ocular Reflex Adaptation. Journal of the Association for Research in Otolaryngology, 21, 277–285. https://doi.org/10.1007/s10162-020-00751-6 Cited by: 12
Meldrum, D., Kearney, H., Hutchinson, S., McCarthy, S., & Quinn, G. (2024). Wearable sensor and smartphone assisted vestibular physical therapy for multiple sclerosis: usability and outcomes. Frontiers in Rehabilitation Sciences, 5. https://doi.org/10.3389/fresc.2024.1406926 Cited by: 8
Prell, T., & Axer, H. (2022). Avoidance Behavior in Patients with Chronic Dizziness: A Prospective Observational Study. Journal of Clinical Medicine, 11, 7473. https://doi.org/10.3390/jcm11247473 Cited by: 6
Van Laer, L., Dunlap, P. M., Vereeck, L., Hendriks, E., Sluydts, M., & Whitney, S. L. (2023). Fear avoidance beliefs, anxiety, and depression in healthy individuals and persons with vestibular disorders across cultures. Frontiers in Neurology, 14. https://doi.org/10.3389/fneur.2023.1296411 Cited by: 10
Wang, L., Zobeiri, O. A., Millar, J. L., Souza Silva, W., Schubert, M. C., & Cullen, K. E. (2021). Continuous Head Motion is a Greater Motor Control Challenge than Transient Head Motion in Patients with Loss of Vestibular Function. Neurorehabilitation and Neural Repair, 35, 890–902. https://doi.org/10.1177/15459683211034758 Cited by: 9